How heart failure leads to water retention and low serum sodium
The pathophysiology of heart failure and its relationship to hyponatremia is complex, as depicted in the figure below.
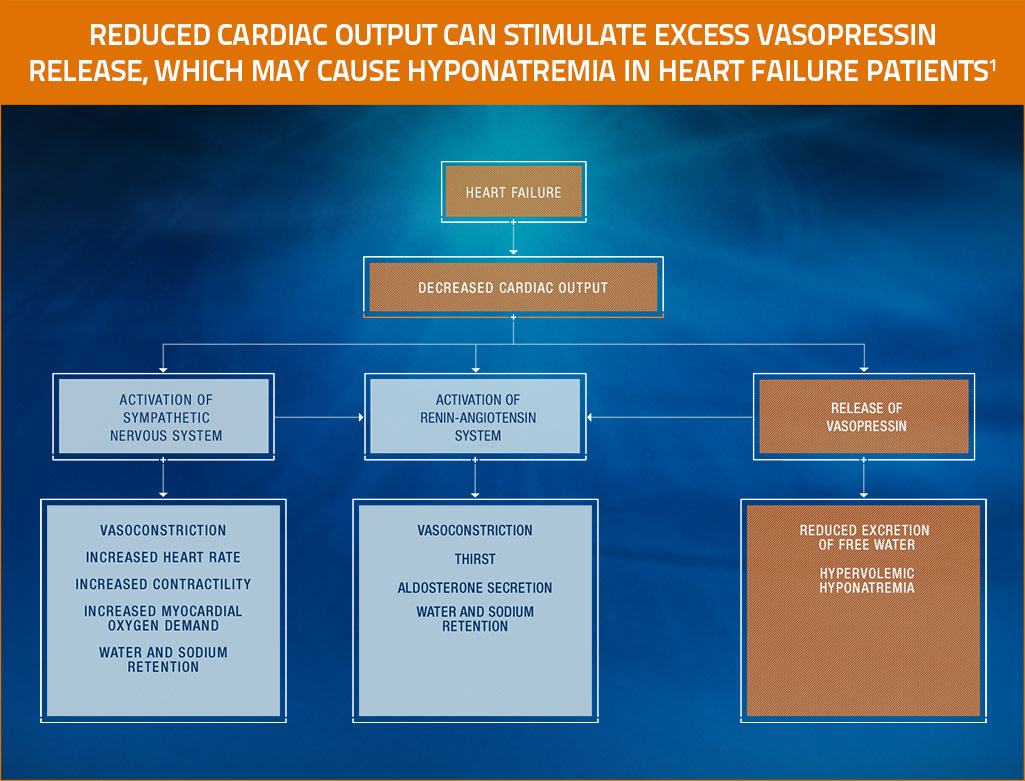
Derived from Mann, Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 2012.1
Role of vasopressin in hyponatremia in heart failure
- Reduced cardiac output in heart failure stimulates the release of vasopressin, resulting in elevated levels of circulating vasopressin1
- Because vasopressin reduces the excretion of free water, elevated levels of vasopressin may contribute to the development of hyponatremia in heart failure patients1
Role of renin-angiotensin-aldosterone system in hyponatremia in heart failure
- Reduced cardiac output and decreased renal perfusion activates the renin-angiotensin-aldosterone system in heart failure patients1,2
- The excess of angiotensin II in heart failure causes the following which further exacerbate dilutional hyponatremia1,3:
- systemic and arteriolar vasoconstriction
- increase in aldosterone concentration
- increased thirst
- In heart failure, water and sodium retention occur in response to aldosterone2